By the numbers
We help customers reduce waste with product size optimization.
Based on hospitals analyzed, we found institutions benefited in these areas*:
2,066,619
Over Two Million Waste Transactions Identified
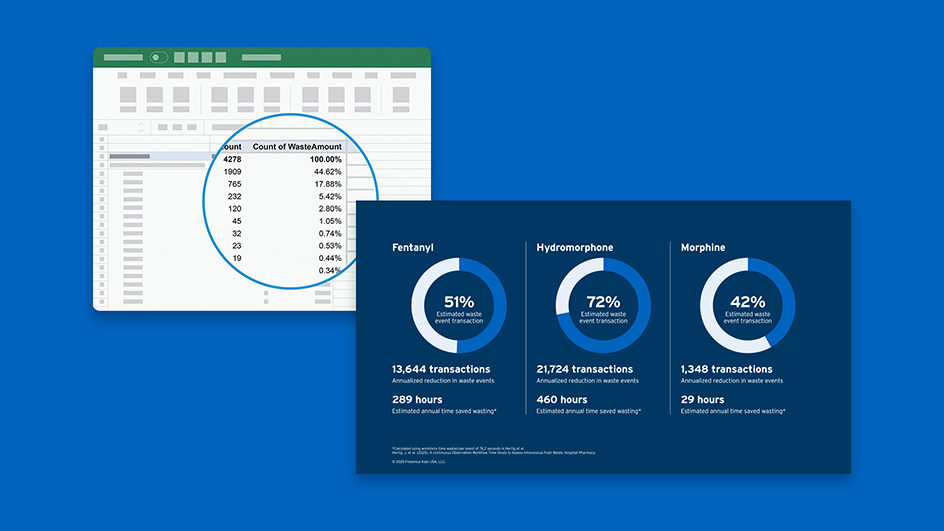
Fentanyl (n = 176)
Hydromorphone (n = 181)
Morphine (n = 155)
53%
Estimated average annual waste event reductions
461,049 transactions
Estimated annual waste event reductions
9,759 hours
Estimated annual time saved*
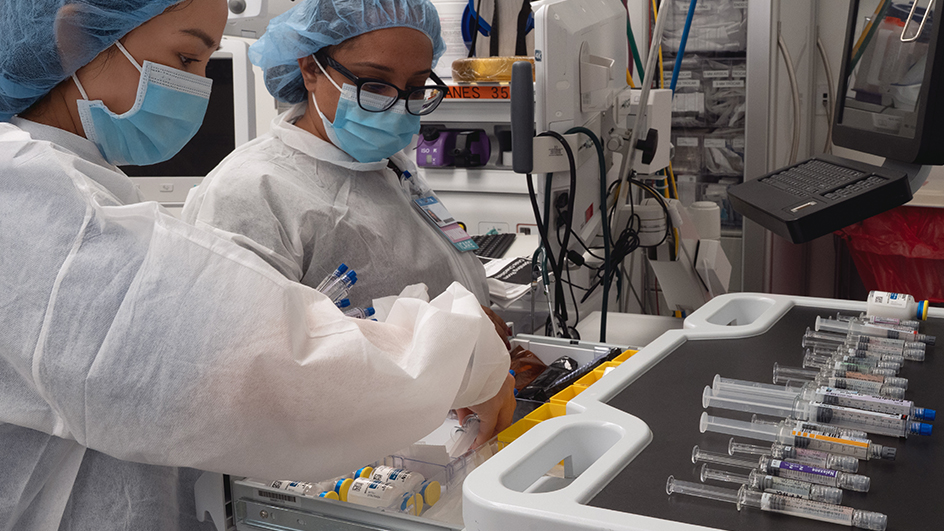
Waste Events
Healthcare providers must discard any excess controlled substances if the quantity dispensed exceeds the prescribed dose. Hospital protocols may differ on how this procedure is carried out.
Data Ananlysis Process
By analyzing data from previous instances of waste in healthcare facilities, it is possible to calculate potential reductions by aligning product size with clinical practice.
*Data on file provided by real clients. Hospitals analyzed N = 183, Fentanyl Citrate Injection, USP n = 176, Hydromorphone HCI Injection, USP n = 181, Morphine Sulfate Injection, USP n = 155.
Fresenius Kabi provides no guarantee of the likelihood that you will achieve similar results if you use our products.
Estimated annual time saved reflects one nurse’s time to waste and does not include witness time required.
Calculate the cost of narcotic waste in your institution
-
Upload your automated dispensing cabinet waste report
Simple, anonymous, and secure.
-
Get instant analysis of controlled substance waste
See product-level waste and diversion insights within minutes.
-
Discover opportunities to reduce diversion risk and time
Use the report to implement change, and request a full consultation with the Director of Integrated Pharmacy Solutions for deeper analysis.
Simplist is associated with a 4x lower error rate* compared to traditional practice, including a cartridge-based syringe system3
*A prospective, multisite, observational study of IV push medication preparation and administration compared the error rates between ready-to-administer products and traditional practice, including a cartridge-based syringe system and vial and syringe. Simplist was the only RTA delivery system used in the study. Study limitations include only a select number of sites (3) and steps observed.
Less preparationDiscover Simplist













Talk to a representative
For questions about Simplist®, our products, or ordering, please complete the form below so a representative can best assist you.
Customer Support
Please contact our Customer Service Department, Monday through Friday, 7:00AM – 6:00PM (CST) at:
Toll-Free: (800) 386-1300
For additional product information or to place an order, please contact your Sales Representative.
Medical Affairs
If you have a question regarding any of our products, please contact the Fresenius Kabi Medical Affairs Department Monday through Friday, 8:00AM – 5:00PM (CST) at:
Toll-Free: (800) 551-7176